

Ioannis K. Raptis is a certified physician (MIC II title) for performing advanced laparoscopic and hysteroscopic procedures, accredited by the German Society for Gynecological Endoscopy (AGE). For the majority of patients, laparoscopic and robotic procedures are offered without hospitalization.
Follow us

Uterine fibroids are a very common benign condition that mainly affects women of reproductive age.
This condition occurs in up to 80% of women by the age of 50.
The following comprehensive guide aims to provide detailed information about the types, causes, symptoms, safe treatment, and other important issues related to uterine fibroids.
Contents:
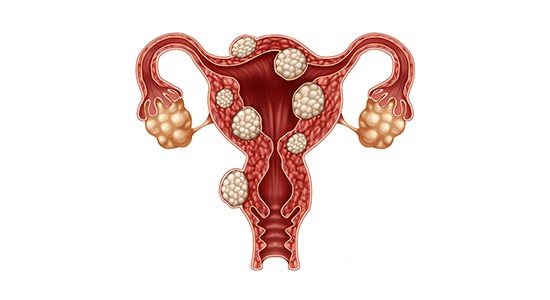
Uterine fibroids are benign tumors of the wall of the uterus, the growth of which may extend either toward the uterine cavity or outward beyond the organ.
They are solid masses composed of muscular and fibrous tissue which, depending on their size and location, may cause various symptoms.
Fibroids usually grow gradually, although in some cases they may increase in size more rapidly.
Their development is stimulated by female hormones (estrogens), which is why they tend to regress after menopause.

The exact cause of their development is not fully known. However, the growth of fibroids appears to be stimulated by female hormones (primarily estradiol).
Therefore, fibroids mainly affect women of reproductive age, and the likelihood of developing them increases in overweight women (as adipose tissue produces estrogens).
For the same reason, fibroids often increase in size during pregnancy. Conversely, after menopause they tend to shrink, as estrogen levels significantly decrease during this period.
A family history of fibroids increases the likelihood of their occurrence. At the same time, fibroids are more common in women of African descent. **This indicates that fibroids also have a genetic basis.**
Nowadays, it has also been observed that the development of fibroids in younger women may be associated with **modern dietary habits**, including limited intake of fruits, vegetables, and vitamin D.
Depending on their location, uterine fibroids are classified into three categories:
When the largest portion of the fibroid is located on the outer surface of the uterine wall, it is referred to as a subserosal fibroid. In general, these cause symptoms once they grow to a considerable size (5–6 cm).
They exert pressure on the surrounding tissues of the uterus, such as the bladder and the intestines, leading to disturbances in urination, bowel movements, or sexual intercourse.
If the fibroid has a very thin stalk, there is a risk of torsion, which may cause sudden and severe abdominal pain.

Intramural (or mural) fibroids are those whose largest portion is located within the muscular wall of the uterus. This is the most common type of fibroid.
When their size exceeds 2–3 cm, they may interfere with the normal contraction of the uterus during menstruation, leading to heavy bleeding or pain.
If they distort the uterine cavity, they may cause infertility or, more commonly, recurrent miscarriages.
In addition to their size, the number of fibroids also plays an important role, as symptoms tend to worsen as their number increases.
Uterine fibroids that protrude into the uterine cavity are associated with more intense symptoms and are referred to as submucosal fibroids.
Even when small in size (1–2 cm), these fibroids may cause heavy bleeding, infertility, and recurrent miscarriages.
This is because they disrupt the function of the endometrium, which plays a key role both in menstruation and in supporting a pregnancy.
The symptoms caused by uterine fibroids vary depending on their size, location within the uterus, and number.
These may include:
It should never be forgotten that, in very rare cases, malignancy may develop within large fibroids.
For this reason, it is extremely important that special protective measures are taken during their removal.
The management of uterine fibroids depends on various factors, such as:
Treatment may be either conservative or surgical.
At an early stage, and provided that the uterine fibroids are small, asymptomatic, and do not cause significant problems, regular monitoring is recommended.
Specifically, fibroids should be evaluated every 6 to 12 months.
There is no definitive medical (drug) therapy for the treatment of fibroids. Oral contraceptive pills, which were previously prescribed for this condition, have now been shown to potentially stimulate rather than resolve the problem.
Medications with some therapeutic effect (e.g. Esmya, GnRH analogues) are mainly administered preoperatively for temporary symptom control.
In perimenopausal women, such medications may be used for a short period in cases of moderate symptoms, bridging the time until menopause, when fibroid regression and shrinkage are expected.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
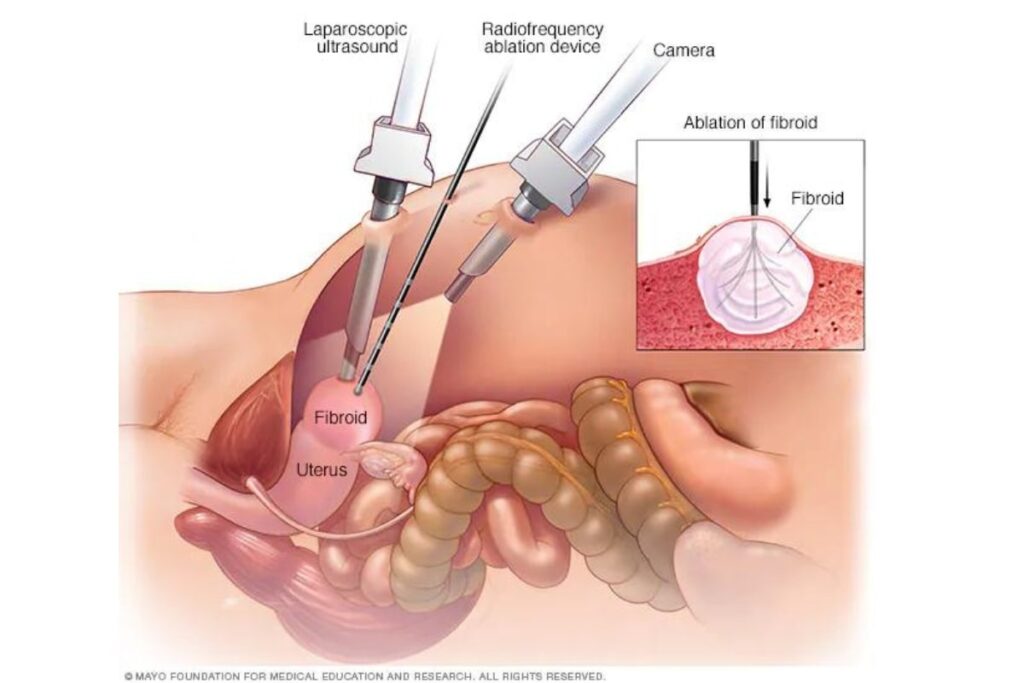
Uterine fibroids can be removed in the vast majority of cases endoscopically through myomectomy (hysteroscopic, laparoscopic, or robotic).
When the condition is very extensive and the patient has completed her family planning, removal of the uterus (hysterectomy) provides a definitive solution.
Laparoscopy is nowadays considered the safest, most effective, and minimally invasive method for resolving the problem and restoring proper uterine function through extremely small abdominal incisions with the assistance of an endoscope.
When fibroids protrude into the uterine cavity, they can be removed hysteroscopically. This is performed through the natural vaginal route and the entrance of the uterus, using a very thin camera and specialized micro-instruments.
In women over 40 years of age who have completed their family planning or have developed multiple and large fibroids, hysterectomy is indicated as the surgical treatment of choice.
Hysterectomy includes removal of the uterine body (without the cervix) or removal of the entire uterus (subtotal and total hysterectomy respectively).
If the patient is not in menopause, the ovaries can remain in place, resulting in no hormonal changes.
In other words, although patients will no longer have a menstrual period, they are not in menopause and continue to produce hormones normally.
Hysterectomy can be performed laparoscopically, more rarely vaginally, and in only a few cases abdominally.
The advantages of laparoscopic fibroid removal compared to the outdated classical abdominal incision include the following:
Nowadays, the specialized training of modern endoscopic surgeons in international centers has established laparoscopy as the first-line treatment for almost the entire spectrum of gynecological conditions.
In approximately 1 out of 500 women undergoing laparoscopic myomectomy, an underlying malignant fibroid (sarcoma) may be present.
In such cases, due to the fragmentation of the fibroid within the abdominal cavity (in order to remove it through the small laparoscopic incisions), there is a significant risk of spreading the malignancy inside the abdomen, potentially with serious implications for the prognosis of the disease.
The same risk applies in cases of laparoscopic supracervical hysterectomy.
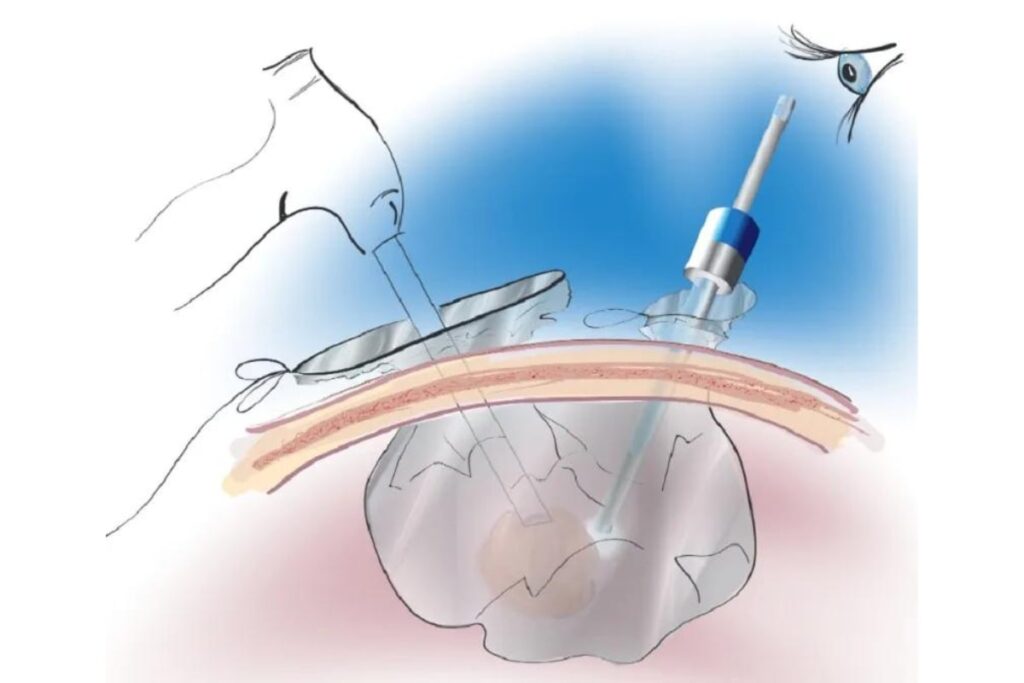
As early as 2014, the U.S. Food and Drug Administration (FDA) issued a directive prohibiting unprotected tissue morcellation in women undergoing laparoscopic fibroid removal or supracervical hysterectomy.
In order for patients to continue benefiting from the undeniable advantages of laparoscopic surgery without compromising their safety through unprotected morcellation, a special closed containment bag system is always used.
This system is introduced into the abdominal cavity through the laparoscopic ports, and the fragmentation of the fibroids takes place inside it, ensuring protection and eliminating the risk of spreading a potential malignancy.
The same system must also be used in cases of laparoscopic supracervical hysterectomy.
The application of this system is specialized and requires appropriate surgical expertise.
For more information, click here.
Preventing the development of uterine fibroids requires changes in dietary habits in order to maintain estrogen levels within normal range, achieve hormonal balance, and reduce inflammatory processes.
Your diet should ideally include the following:
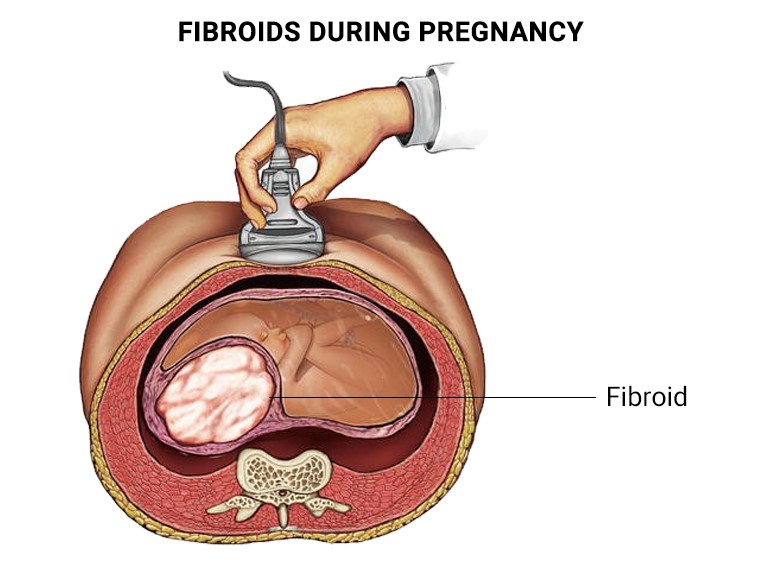
The presence of fibroids often creates difficulties in conception and in maintaining a pregnancy, mainly due to anatomical distortions of the uterine cavity.
The most common complications that uterine fibroids may cause during pregnancy include:
The diagnosis of uterine fibroids is often made through a bimanual pelvic examination during a gynecological check-up.
Ultrasound examination, and in certain cases magnetic resonance imaging (MRI), help accurately determine their size, location, and number.
The aim of minimally invasive endoscopic microsurgical procedures is the safe and complete removal of fibroids, the elimination of symptoms, and the restoration of the uterus’ anatomy and fertility in younger women.
The procedures are performed under general anesthesia and may last from a few minutes to several hours, depending on the extent of the condition. The patient can usually leave the clinic the same day or the following day.
Full recovery typically takes about 48 hours, after which the patient can return to her normal daily activities. Discomfort during this period is minimal.
We must not forget that it is not the removal of uterine fibroids or other pathologies itself that determines the long-term outcome, but rather the surgical technique and the surgeon’s expertise, which ultimately define the long-term health of the operated organ and, consequently, the patient’s reproductive capacity.
Within this context, the certified specialization of the surgeon plays a decisive role in accurate diagnosis, proper preoperative preparation, and the appropriate application of minimally invasive techniques aimed at avoiding damage to healthy tissues and preserving — as well as supporting — the patient’s fertility.

Χρησιμοποιούμε cookies για να βελτιώσουμε την εμπειρία σας στον ιστότοπό μας. Χρησιμοποιώντας τον ιστότοπό μας, συναινείτε στη χρήση cookies.
Manage your cookie preferences below:
Essential cookies enable basic functions and are necessary for the proper function of the website.