

Ioannis Raptis
MIC II, DEGUM I, AGUB I
Obstetrician – Gynecologist
Ioannis K. Raptis is a certified physician (MIC II title) for performing advanced laparoscopic and hysteroscopic procedures, accredited by the German Society for Gynecological Endoscopy (AGE). For the majority of patients, minimally invasive laparoscopic and robotic procedures are offered without the need for hospitalization.
Follow us

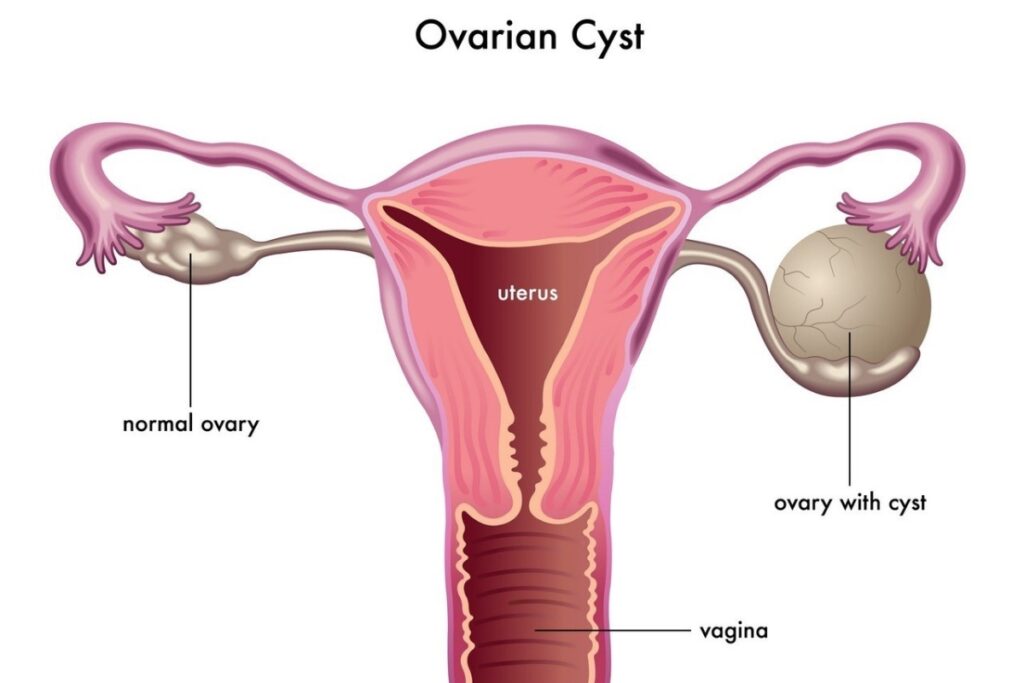
Ovarian Cysts
Ovarian cysts are a common gynecological finding that rarely pose a risk to a woman’s health.
More specifically, they are fluid-filled sacs of varying sizes located within the ovary. In rare cases, an ovarian cyst may also contain solid components in addition to fluid.
The majority of women will develop a cyst at some point in their lives, which in most cases will either resolve or rupture spontaneously without ultimately affecting their health.
However, in certain cases, an ovarian cystic formation may conceal an underlying pathology that requires specialized therapeutic intervention.
For a better understanding of ovarian cysts, it is essential to first understand the function of the ovaries themselves.
The ovaries are among the most important organs of the female reproductive system. Every woman has two ovaries, located outside the uterus, and they are responsible for the following critical functions:
- Production of female hormones (estrogen, progesterone)
- Production of eggs (ovulation) for the purpose of fertilization
Contents:
Ovarian Cysts – Causes
- Failure of follicle rupture (simply put, an egg that did not ovulate)
- Failure of corpus luteum regression (a cyst that forms after ovulation)
- Pregnancy
- Implantation of endometrial tissue in the ovaries (endometrioma)
- Congenital ovarian cysts (e.g., dermoid cyst)
- Rare cysts (stromal or germ cell ovarian cysts)
- Malignancy
- Abscesses
.
Types of Ovarian Cysts
The two main types of ovarian cysts are functional cysts (benign, which in most cases resolve on their own) and non-functional (benign or malignant, which do not resolve spontaneously).
Functional Ovarian Cysts
The formation of a functional cyst is most often related to the failure of the egg to be released (follicular cyst) or to the failure of the sac that forms after ovulation to regress (corpus luteum cyst).
They usually do not cause problems and resolve on their own within approximately 6–8 weeks without complications.
In rare cases, a functional ovarian cyst may grow significantly, cause intense symptoms (abdominal pain, pain during urination, pain during bowel movements, etc.), or even bleed, making surgical removal necessary.
Non-functional Ovarian Cysts
These cysts are caused by abnormal cellular growth in a part of the ovary.
The most common non-functional ovarian cysts are the following:
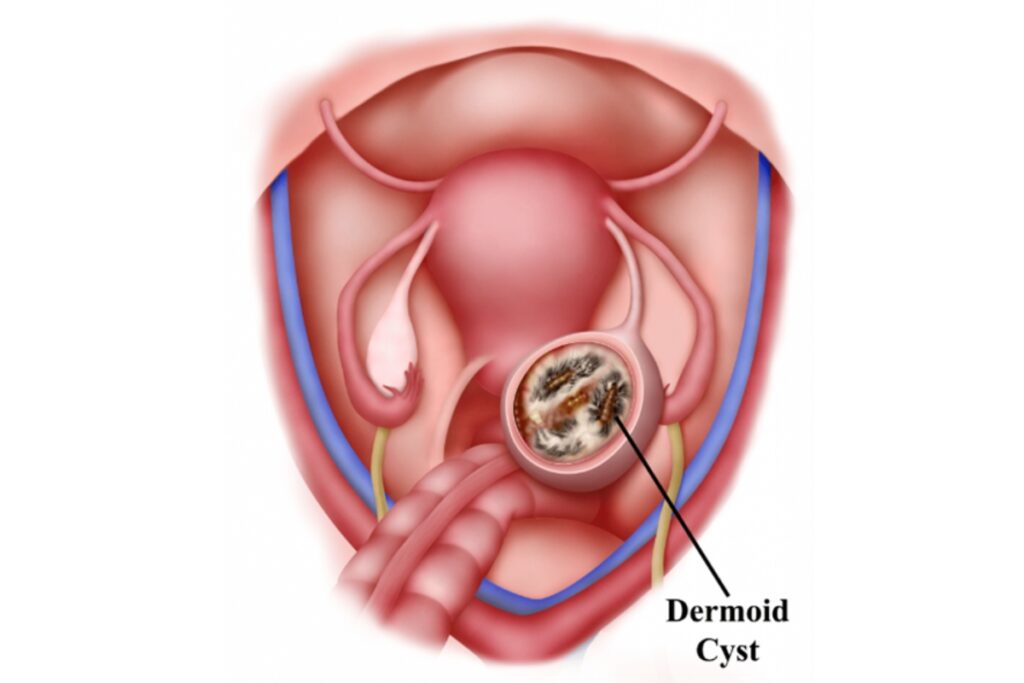
1. Dermoid cyst:
A dermoid cyst is a benign ovarian cyst that may contain various types of tissue, such as hair, fat, teeth, etc. These cysts are not embryonic remnants, as is sometimes mistakenly stated.
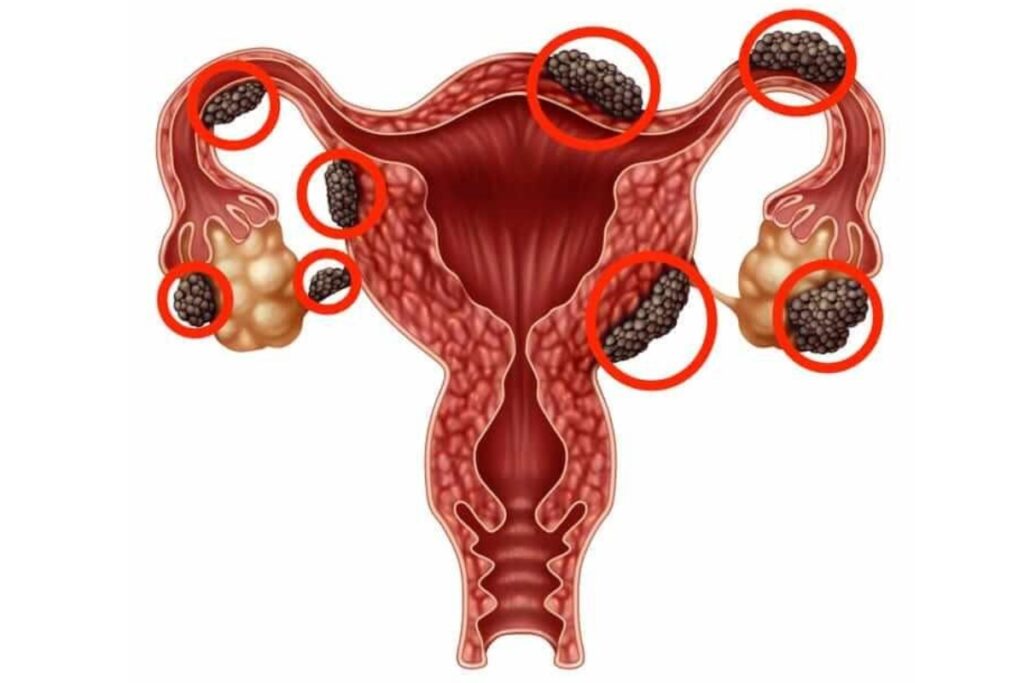
2. Endometriotic cyst (endometrioma):
These cysts develop as a result of implantation of endometrial tissue (the tissue that bleeds during menstruation inside the uterus) in the area of the ovaries.
They are usually associated with severe pain during menstruation and sexual intercourse, and in some cases may lead to infertility.
3. Cystadenomas:
These are benign tumors that develop on the surface of the ovary. They contain either serous (watery) or mucinous fluid.
Ovarian Cysts – Symptoms
For most women, the symptoms of ovarian cysts are not specific, which is why diagnosis may be delayed.
A cyst is mainly associated with symptoms such as:
- Pain in the lower abdomen
- Abdominal pain during exercise or sexual intercourse
- A feeling of abdominal fullness
- Frequent urination
- Pain during bowel movements
- Nausea
- Delayed menstruation
In cases of pressure, rupture, or bleeding of the cyst, the following additional symptoms may occur:
- Lower back pain
- Increase in abdominal circumference
- Abdominal pain with vomiting
- Weakness, tendency to faint
Ovarian Cysts – Diagnosis
The **diagnosis of ovarian cysts** can be made promptly and accurately with a transvaginal ultrasound. Additional imaging tests, such as magnetic resonance imaging (MRI), may provide further information; however, they are not superior to ultrasound.
In cases of suspected complex cysts or malignancy, specialized blood tests may also contribute to the differential diagnosis.
Possible Complications of Ovarian Cysts
An ovarian cyst, primarily when large in size (over 5 cm), may lead to some of the following complications:
- Rupture: An ovarian cyst may rupture, allowing fluid to escape into the abdominal cavity, causing acute abdominal pain, nausea, faintness, etc. In most cases, the pain subsides shortly afterward and the fluid is completely absorbed.
- Bleeding: Hemorrhage may occur due to rupture of blood vessels within the cyst wall, either inside the cyst cavity or into the abdominal cavity.
- Inflammation: In some cases, rupture of a cyst may cause chemical inflammation inside the abdomen, which is not related to the presence of microbes (aseptic inflammation).
- Ovarian torsion: A large cyst may, in rare cases, cause the ovary to twist around its vascular pedicle. In this situation, emergency surgical intervention is required, as there is a risk of ovarian necrosis.
- Infertility: Ovarian cystic formations often occupy significant functional space, making ovulation more difficult.
Ovarian Cysts – Treatment
Conservative Treatment
No treatment is required for functional ovarian cysts, as they usually resolve on their own. The use of oral contraceptive pills or antibiotics for the treatment of an ovarian cyst has no scientific basis.
According to all studies, any regression of cysts observed during the use of the above medications is purely coincidental.
For mild abdominal discomfort, your doctor may recommend common pain relievers. Otherwise, it is important to avoid physical strain, which may cause additional pain or torsion in cases of large cysts.
Surgical Management of Ovarian Cysts
Surgical removal of ovarian cysts is, in most cases, a minimally invasive therapeutic option. It is usually indicated in cases of non-functional cysts, severe pain, increasing size, or infertility.
Depending on the size of the cyst and the ultrasound findings, the type of surgical procedure for its removal is determined. The surgical techniques used include the following:
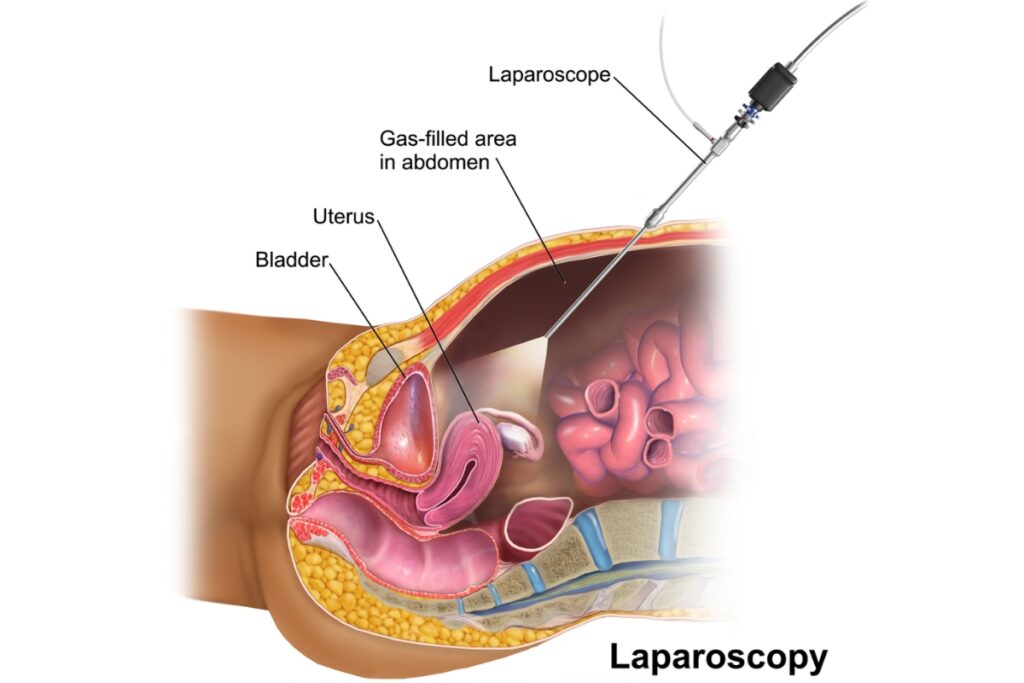
1. Laparoscopic Ovarian Cyst Removal
Today, the surgical treatment of ovarian cysts should, in the vast majority of cases, be performed endoscopically.
With the help of an endoscopic camera and micro-instruments inserted into the abdominal cavity through very small incisions, any cystic formation can be removed with maximum safety.
The advantage of laparoscopic cyst removal compared to the outdated conventional abdominal incision lies in the more radical removal of pathology without damaging healthy tissues, excellent aesthetic results, faster patient mobilization, reduced hospital stay, minimized postoperative pain, and avoidance of postoperative complications such as infections and wound healing disorders.
The endoscopic approach ensures long-term ovarian functionality, optimally protecting the patient’s fertility.
2. Laparotomy
With the conventional laparotomy approach, general anesthesia is administered, followed by a transverse or vertical abdominal incision measuring 12–20 cm.
This approach is recommended only for cysts of very large size.
Frequently Asked Questions
I frequently develop ovarian cysts. What can I do?
In women who tend to develop functional ovarian cysts, the use of oral contraceptive pills can be an excellent way to prevent this specific problem.
Do ovarian cysts affect fertility?
When ovarian cysts are large, they occupy a significant portion of the functional ovarian tissue, impair normal ovarian function, and make the process of ovulation more difficult. In this way, they can directly negatively affect a woman’s fertility.
How can I know which doctor is qualified to perform a laparoscopic ovarian cyst removal surgery?
Endoscopic surgery is a distinct, long-term subspecialty within gynecology, which is officially certified by the respective healthcare system in the form of a DIPLOMA or MEDICAL TITLE.
For this reason, the selection of the appropriate gynecologist to perform a laparoscopic procedure should take into account their certified subspecialty qualifications as well as their clinical (practical) experience.
According to the scientific standards
of the German Society of Obstetrics and Gynecology
