

Ioannis Raptis is a former Senior Consultant (Attending A’) and Head of the Laparoscopic Department at the German academic hospital AKH Hagen. He is a certified physician (MIC II qualification) authorized to perform advanced laparoscopic and hysteroscopic procedures of high complexity by the German Society for Gynecological Endoscopy (AGE).
Follow Us

Laparoscopy is a modern surgical technique that allows endoscopic access to the internal organs of the abdomen and enables the treatment of a wide range of conditions while avoiding the traditional abdominal incision.
It represents the most important technique of **Minimally Invasive Surgery**, offering multiple comparative advantages over the conventional open approach.
With the help of laparoscopy, patients can achieve accurate diagnosis or effective treatment of their condition while minimizing the risk of complications and ensuring the best possible aesthetic outcome.
In gynecology, laparoscopic surgery is performed exclusively by specialized endoscopic surgeons – obstetrician-gynecologists who have received appropriate training and hold certified laparoscopic expertise.
Below, you will find all the necessary information regarding laparoscopic gynecological surgery, its benefits, as well as the stages of preparation and recovery.
Contents:
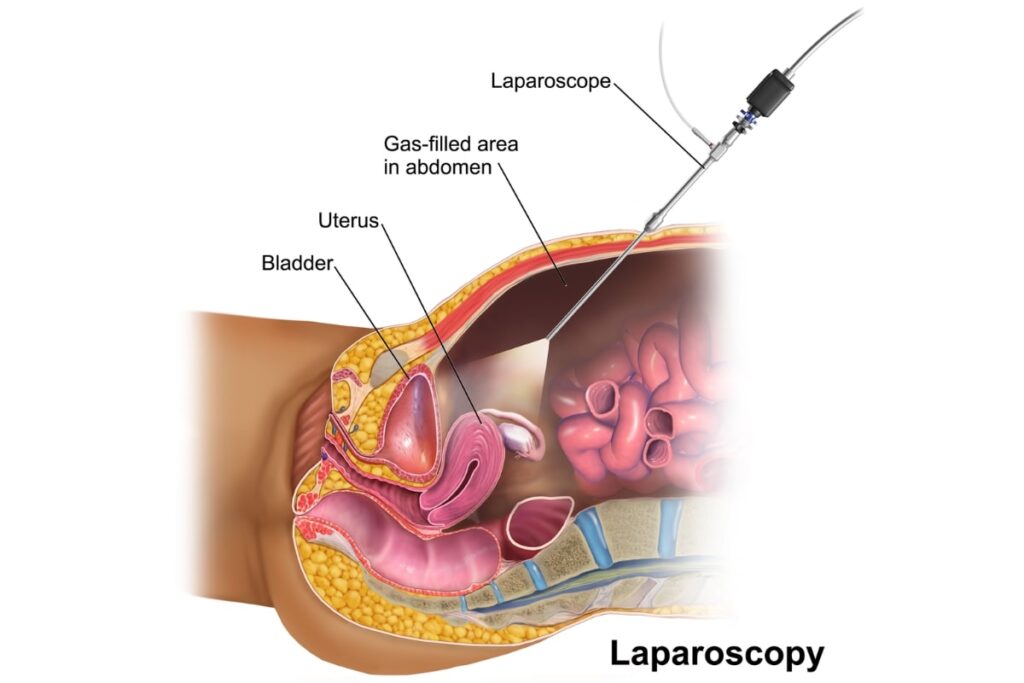
Laparoscopy is a surgical technique that involves performing procedures using a specialized endoscopic camera and fine microsurgical instruments, which are inserted into the human body through small incisions on the abdominal surface.
In gynecology, laparoscopy serves both as a diagnostic tool (diagnostic laparoscopy) and as a therapeutic method for the treatment of various conditions (operative laparoscopy).

The most common conditions that require laparoscopy are the following:
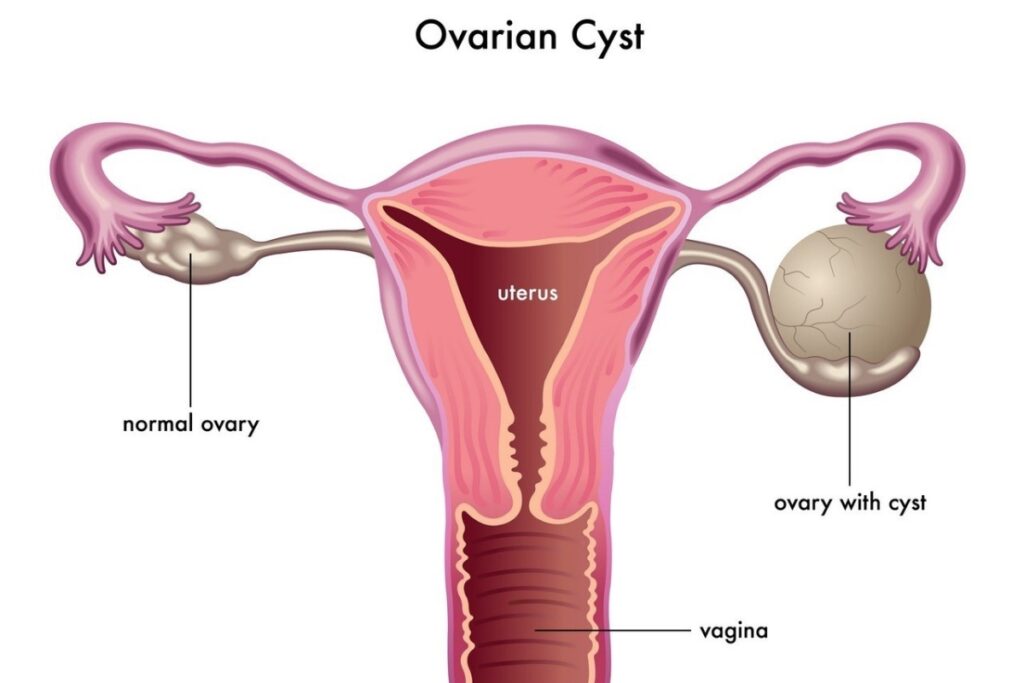
Ovarian cysts are cystic formations that vary in texture, size, and histological identity.
Ovarian cysts may be functional. These almost always resolve spontaneously without the need for surgical intervention.
However, there are also complex ovarian cysts, which have a thick wall, cannot regress on their own, and may affect ovarian function or threaten the patient’s health. In such cases, surgical removal is required.
Laparoscopic ovarian cyst removal ensures radical, bloodless excision of the lesion with maximum preservation of the remaining healthy ovarian tissue and, consequently, the patient’s reproductive capacity.
After laparoscopic ovarian cyst removal, hospitalization is not required. The procedure is performed under general anesthesia, and recovery typically lasts 1–2 days.
Endometriosis is defined as the growth of endometrial tissue (the lining of the uterine cavity) in areas of the abdomen outside the uterus, primarily causing severe menstrual pain, pain during sexual intercourse, and in rare cases, problems affecting other abdominal organs such as the bowel, ureters, ovaries, etc.
During laparoscopy, laser vaporization, cauterization, or excision of endometriotic lesions is performed with maximum precision, aiming at the complete eradication of the disease.
Following laparoscopic removal of endometriosis, injectable medical therapy for 3 to 6 months may be recommended, reducing the likelihood of disease recurrence. Alternatively, oral medications may be prescribed for a longer period.
Laparoscopic removal of endometriosis usually requires an overnight stay at the clinic. The duration of recovery depends on the extent of the condition and typically ranges from 1 to 5 days.
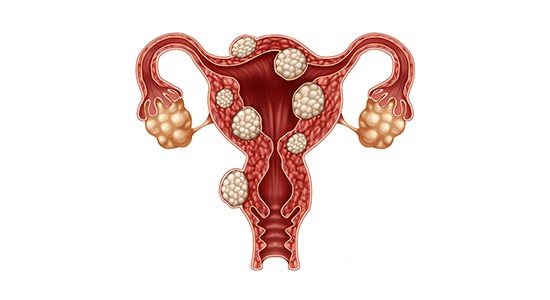

In the vast majority of cases, their removal is performed endoscopically. This approach ensures radical excision of the lesion and the lowest possible risk of recurrence.
However, in approximately 1 in 300 women undergoing laparoscopic myomectomy, an underlying malignant fibroid (sarcoma) may be present.
In such cases, due to the fragmentation of the fibroid within the abdominal cavity (in order to remove it through the small incisions), there is a significant risk of spreading the malignancy inside the patient’s abdomen, potentially with serious implications for the prognosis of the disease.
For this reason, during laparoscopic removal of fibroids, the use of a special closed containment bag system is mandatory.
This system is introduced into the abdominal cavity through the laparoscopic ports, and fragmentation of the
fibroids
takes place within it, ensuring protection and eliminating the risk of spreading a potential malignancy. The same system must also be used in cases of laparoscopic supracervical hysterectomy.
Laparoscopic removal of fibroids usually requires an overnight stay at the clinic. Recovery lasts 1–2 days. Pregnancy should be avoided for six months following the surgical procedure.
In cases of infertility of unknown etiology (approximately 50% of infertile couples),
laparoscopy may contribute decisively to the effort to achieve pregnancy
.
According to research, in approximately 80% of women with unexplained infertility, underlying pathologies are present that cannot be diagnosed with conventional examinations.
The most common of these are endometriosis, chronic asymptomatic abdominal inflammation, intra-abdominal adhesions, and polycystic ovary syndrome. In such cases, every aggravating factor can be treated accurately and painlessly through the laparoscopic approach.
According to studies, following laparoscopy, 25% of couples with infertility of unknown etiology achieve pregnancy through natural intercourse without any assisted reproduction, while for the remaining couples, the success rates of assisted reproductive methods increase.
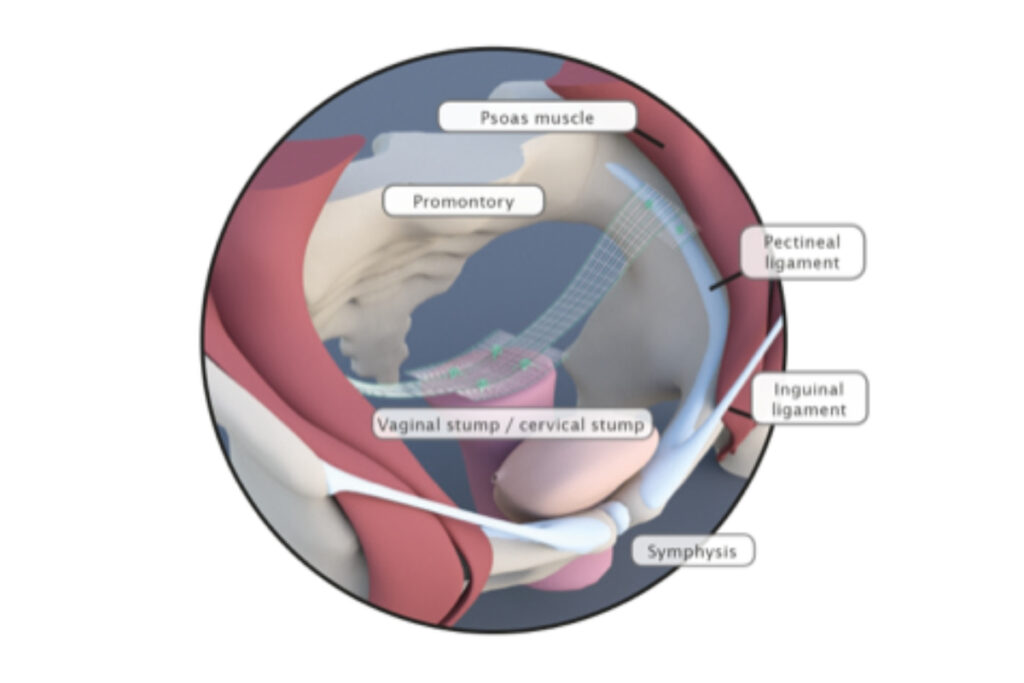
Laparoscopic pectopexy (Pectopexy) is the most modern method of laparoscopic repair for
uterine and vaginal prolapse.
Through laparoscopic pectopexy, elevation of the vagina is achieved with the use of a mesh, without the risk of bleeding and postoperative discomfort associated with the classical technique (laparoscopic sacropexy).
This technique has the advantage that it can be safely applied even in overweight patients. At the same time, the laparoscopic approach ensures minimal surgical burden, rapid return to normal activities, and excellent aesthetic results.
The laparoscopic approach is the method of choice for the removal of the uterus in order to treat various gynecological conditions.
Laparoscopic hysterectomy
involves removal of the uterus with or without its adnexa (ovaries and fallopian tubes), depending on the patient’s age and the indication for surgery.
The use of the endoscopic approach and the avoidance of the traditional abdominal incision have been proven to maximize surgical outcomes, reduce the likelihood of complications, and minimize the burden on the patient, who fully recovers within 1–2 days.
Laparoscopic hysterectomy, with or without lymph node removal, is the most established method for patients with uterine cancer.
This is due to the clearly lower rate of intraoperative (organ injury, bleeding, etc.) and immediate postoperative (infections, wound contamination, etc.) complications compared to the traditional open approach.
At the same time, patient recovery is significantly faster than with a conventional open incision, which, among other benefits, allows for the prompt initiation of any necessary adjuvant therapy (chemotherapy).
General anesthesia is required for a laparoscopic procedure, ensuring that the patient remains completely unaware of the entire process.
During laparoscopic surgery, a specialized endoscopic camera and fine microsurgical instruments are used. These are inserted through very small incisions (0.5 to 1 cm) in the abdominal area. The incisions are almost always made in the region of the navel and the pubic area.
Adequate visibility is achieved by insufflating the abdomen with warm carbon dioxide (CO₂), which is removed at the end of the procedure. Visualization is performed using high-definition cameras and monitors, and at the conclusion of the surgery, the patient receives a video recording of the entire procedure.
The tissues removed during surgery are extracted through the small incisions. If they are large (e.g., a sizeable fibroid), they are fragmented within the abdominal cavity, always in a protected manner using a special containment bag.
The laparoscopic approach offers numerous significant benefits compared to the traditional open technique.
The main advantages of laparoscopy are the following:
Preparation for a gynecological laparoscopic procedure begins a few days in advance with the preoperative evaluation at the clinic.
This usually includes blood tests and a cardiology assessment, while the patient does not need to be fasting at that time.
In the days leading up to the procedure, special attention is given to proper bowel preparation, as the bowel should not be distended on the day of surgery.
For this reason, the patient is advised for 3–4 days to avoid, as much as possible, the consumption of legumes, vegetables, and dairy products.
The day before the procedure, the intake of a laxative is usually recommended to empty the bowel, and adequate fluid intake is important.
During the last 8 hours before surgery, the patient must remain fasting and avoid consuming any food or liquids.
Recovery after a laparoscopic procedure is short, and in the vast majority of cases, the patient is discharged the same or the following day.
During the first 1–2 days after surgery, mild weakness may occur as a result of general anesthesia.
In most patients, pain ranges from minimal to absent. In case of discomfort, standard analgesic medications are administered.
A mild sensation of bloating is normal, due to small residual amounts of air within the abdominal cavity, and resolves within a few days after the procedure.
Adequate fluid intake, early mobilization, chewing gum, and possibly the use of mild laxatives help stimulate bowel function, which should be restored within the first 3 days after surgery.
The patient returns promptly to her daily activities unless otherwise instructed by the attending physician.
General anesthesia is administered for a laparoscopic procedure. Therefore, the patient is completely unable to perceive anything during the operation.
The cost of laparoscopy varies depending on the physician, the hospital/clinic, and the indication for which it is performed.
The closure of the small incisions is performed using special absorbable sutures, which are not visible and do not require removal.
Showering at home is permitted from the day of the procedure. After showering, it is important for the patient to thoroughly dry the incisions to ensure an optimal aesthetic result.
During the first postoperative week, it is advisable to avoid any significant physical exertion in order to prevent abdominal pain.
After completion of the procedure, the surgical instruments and the air from inside the abdominal cavity are removed.
In rare cases, a small amount of air may remain trapped. However, it is absorbed during the immediate postoperative period.
