

Ioannis Raptis
MIC II, DEGUM I, AGUB I
Obstetrician – Gynecologist
At the medical practice of Ioannis Raptis, infertility issues are managed in accordance with the guidelines of the “Frankfurt Hormone School” (Frankfurter Hormonschule) and the International Society of Gynecological Endocrinology (ISGE).
Follow us

Laparoscopy and Infertility
There are many cases in which a couple’s desire to have a child remains unfulfilled, even though clinical and laboratory findings are normal and no specific underlying cause can be identified.
In other cases, conditions such as ovarian cysts, endometriosis, fibroids, abdominal adhesions, polycystic ovary syndrome (PCOS), abnormalities of the uterine cavity, and endometrial disorders constitute significant factors that negatively affect a woman’s fertility.
Many of these conditions may remain undiagnosed for a long period of time, complicating the efforts of both patients and physicians.
Today, with the help of modern endoscopic techniques, we are able to directly visualize all the organs and structures involved in the fertilization process, assess their patency, examine their condition, and at the same time effectively and precisely treat any problems that may be identified.
Moreover, the minimally invasive nature of these methods ensures the least possible burden on the patient and her healthy tissues.
What endoscopic methods are available?
There are two main methods: laparoscopy and hysteroscopy.
With laparoscopy, we are able to visualize the organs inside the abdominal cavity—particularly within the female pelvis—using a camera. With the help of specialized instruments, any existing pathologies can also be treated.
All instruments are inserted into the abdominal cavity through very small incisions, only a few millimeters in length, ensuring excellent cosmetic results.
With hysteroscopy, we again use an endoscope to examine the entire natural pathway, starting from the vagina and extending into the uterine cavity and fallopian tubes, assessing their integrity and patency. In this case as well, minor surgical procedures can be performed when necessary, without the need for incisions.

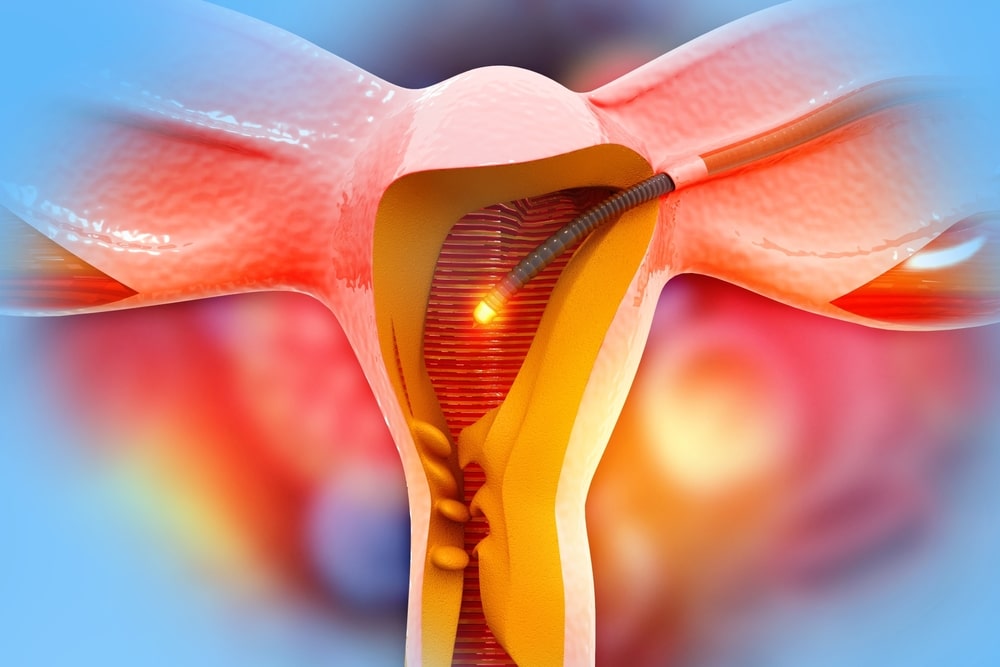
How is tubal patency assessed laparoscopically?
This is done using a special colored dye, which is introduced into the uterine cavity through a catheter. If there is no obstruction, the dye passes from the uterus into the fallopian tubes and then into the abdominal cavity, where it can be observed by the surgeon.
This confirms that there is no mechanical barrier preventing the egg and sperm from meeting, as they begin their journey from the ovaries and the vagina respectively.
What happens if the fallopian tubes are blocked?
In such cases, the underlying cause of the obstruction must be identified and removed.
The blockage may be located within the abdomen (e.g., ovarian cysts, adhesions from previous surgeries or abdominal infections, fibroids, etc.) or within the uterus (e.g., anatomical abnormalities, polyps, adhesions, fibroids, etc.). In either case, surgical treatment can often be performed immediately, significantly increasing the patient’s chances of achieving pregnancy.
What if the problem lies in the fallopian tubes themselves?
When the damage is limited, microsurgical techniques can be used to reopen the fallopian tubes using modern surgical methods.
In cases of extensive tubal damage—such as after a severe past infection—the tube may become non-functional (hydrosalpinx). In such situations, removal is recommended, as the fluid trapped inside the tube may be toxic to the endometrium and significantly reduce the chances of successful conception.
A woman with one functional fallopian tube has nearly the same chances of natural conception as a woman with two healthy tubes.
In the rare case where both tubes must be removed due to irreversible damage (bilateral hydrosalpinx), natural fertilization is no longer possible, and the patient should seek treatment at an assisted reproduction center.
How can a woman with Polycystic Ovary Syndrome (PCOS) and infertility benefit from laparoscopy?
In certain patients with PCOS, conventional treatments may fail to restore hormonal balance and induce regular ovulation, or assisted therapies may not successfully stimulate egg maturation.
In these cases, ovarian drilling—a laparoscopic procedure that creates small openings in a number of immature follicles (cysts) on the ovarian surface—can help reduce androgen levels in the blood. This often leads to more regular ovulation and improved response to stimulation for a period that may last several years after the surgery.


How else can endoscopic methods help a woman with infertility?
Recent research suggests that a percentage of seemingly healthy women—without anatomical, hormonal, or other identifiable abnormalities—may fail to achieve pregnancy because the endometrium itself does not provide a suitable environment for embryo implantation. This may be due to an underlying chronic inflammation or to immunological factors produced by the endometrium.
With the help of hysteroscopy, we can examine the endometrium with exceptional clarity and identify signs that may indicate such abnormalities. At the same time, small endometrial biopsies can be obtained to assess the presence of unfavorable inflammatory or immunological factors.
Finally, hysteroscopic “endometrial scratching” may, according to some studies, improve pregnancy rates in women who are about to undergo in vitro fertilization (IVF).
How long is hospitalization required after an endoscopic procedure?
In the case of diagnostic laparoscopy or hysteroscopy, hospitalization is not required, and the patient is discharged just a few hours after the procedure.
In the case of operative laparoscopy or cystoscopy, and depending on the extent of the surgery, hospitalization may be necessary. However, in the vast majority of cases, it is limited to a one-day stay.
• For laparoscopic ovarian drilling, the new minimally invasive LEROS method (Laparoscopic Elektroresektion of Ovarian Surface) is used.
MEDIA
According to the scientific standards
of the German Society of Obstetrics and Gynecology
